Here’s something that happens to millions of women every month: they’re in pain — real, sometimes debilitating pain — and they’re told it’s “just part of being a woman.” By their mothers, their friends, their doctors. The message is clear: suck it up.
Sometimes that advice is correct. Some cramping during menstruation is normal and expected.
But sometimes it’s not. Sometimes pain is your body’s way of telling you something specific is wrong — something treatable — and the “just deal with it” response is actively harmful medical negligence disguised as cultural wisdom.
So let’s draw a clear line between the two. Not a vague “listen to your body” — a specific, actionable framework for knowing when your cramps are cramps and when they’re a signal.
Why Periods Hurt (The Normal Mechanism)
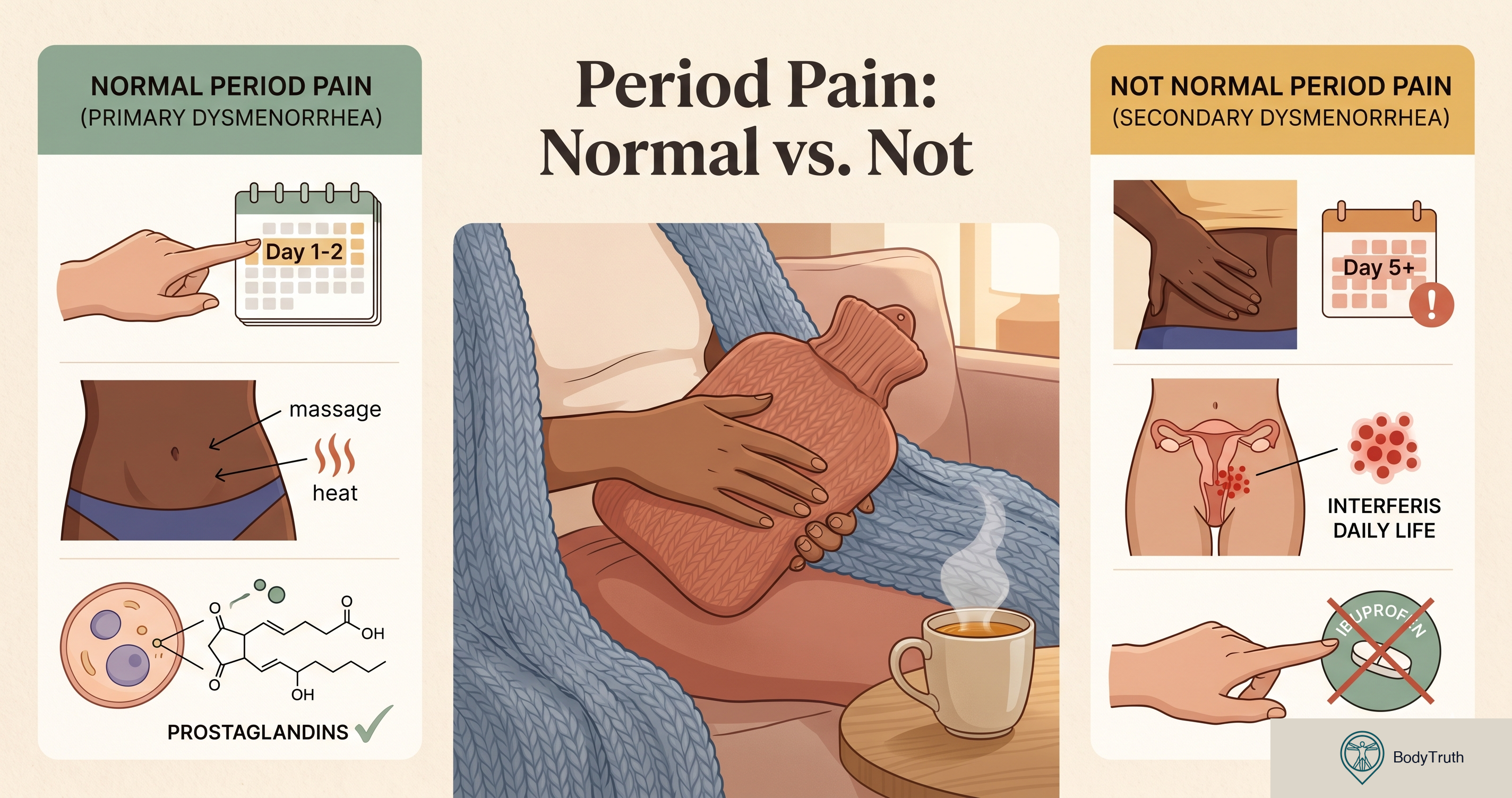
During menstruation, your uterus contracts to shed its lining. These contractions are triggered by prostaglandins — hormone-like chemicals that cause muscle contractions and inflammation. Higher prostaglandin levels = stronger contractions = more pain.
This is called primary dysmenorrhea — period pain that has no underlying disease. It’s the normal kind.
What normal period pain feels like:
- Cramping in the lower abdomen
- Usually starts just before or at the beginning of your period
- Peaks within the first 1–2 days
- Responds to NSAIDs (ibuprofen, naproxen)
- Doesn’t prevent you from functioning entirely
- May include mild lower back pain
- Improves after your early twenties or after childbirth
If this describes your experience — you’re likely in normal territory. It’s not fun, but it’s not pathological.
When Pain Crosses the Line
Secondary dysmenorrhea is period pain caused by an underlying condition. It behaves differently, and ignoring it means leaving a treatable condition unaddressed.
Red flags that suggest something beyond normal cramps:
Severity
- Pain so intense you can’t go to work or school regularly
- Pain that makes you vomit, pass out, or end up in the ER
- Pain that isn’t adequately controlled by standard doses of ibuprofen
- Pain that has gotten progressively worse over months or years
Timing
- Pain that starts well before your period (5–7+ days before)
- Pain that extends well after your period ends
- Pain during ovulation (mid-cycle) that’s severe
- Pain during or after sex (deep penetration pain)
Character
- Sharp, stabbing pain rather than cramping
- Pain on one side only (could indicate ovarian issues)
- Pain during bowel movements or urination during your period
- Pain radiating down your legs
Associated symptoms
- Extremely heavy bleeding (soaking through a pad/tampon every hour for several hours)
- Large blood clots (bigger than a quarter)
- Periods longer than 7 days
- Bleeding between periods
- Difficulty getting pregnant
If several of these apply to you — this isn’t “just cramps.” Keep reading.
Conditions That Cause Abnormal Period Pain
Endometriosis
What it is: Tissue similar to the uterine lining grows outside the uterus — on the ovaries, fallopian tubes, bowel, or elsewhere in the pelvis. This tissue responds to your hormonal cycle, becoming inflamed and painful.
How common: Affects approximately 10% of women of reproductive age. Takes an average of 7–10 years to diagnose because women are told their pain is normal.
Distinctive signs:
- Pain that gets worse over time (progressive)
- Pain during sex (especially deep penetration)
- Pain with bowel movements or urination during periods
- Pain between periods
- Difficulty conceiving
- Fatigue
What helps: Hormonal treatment (birth control, GnRH agonists), excision surgery by a specialist, pain management. It’s manageable but currently incurable.
Adenomyosis
What it is: Similar to endometriosis, but the uterine lining tissue grows INTO the muscular wall of the uterus itself, causing the uterus to enlarge and become painful.
Distinctive signs:
- Extremely heavy, prolonged periods
- Severe cramping throughout the period (not just day 1–2)
- Enlarged, tender uterus
- Often occurs in women 30+
What helps: Hormonal treatment, IUD (Mirena), or in severe cases, hysterectomy.
Fibroids
What it is: Non-cancerous growths in or on the uterus. Very common — up to 70% of women develop fibroids by age 50.
Distinctive signs:
- Very heavy periods
- Periods lasting longer than a week
- Pelvic pressure or fullness
- Frequent urination
- Not always painful — but can cause severe cramping when they’re submucosal (inside the uterine cavity)
What helps: Medication, procedures (embolization, myomectomy), or monitoring if they’re not causing problems.
Ovarian cysts
What it is: Fluid-filled sacs on the ovaries. Most are harmless and resolve on their own. Some cause pain.
Distinctive signs:
- Sudden, sharp pain on one side
- Pain during specific times in the cycle
- Bloating or feeling full quickly
The Diagnosis Gap
Here’s the uncomfortable truth: women’s pain is systematically underdiagnosed and undertreated in medical settings.
Studies consistently show that:
- Women wait longer in emergency rooms before receiving pain medication
- Women’s pain reports are more likely to be attributed to emotional or psychological causes
- Conditions like endometriosis take 7–10 years to diagnose on average
- Many doctors still tell women that severe period pain is “normal”
This means: If your doctor dismisses your pain without investigation, you may need to advocate for yourself. Request an ultrasound. Ask specifically about endometriosis. See a gynecologist (not just a GP). Get a second opinion if the first one doesn’t take you seriously.
You are not being dramatic. You know your own pain better than anyone.
What Actually Helps for Normal Cramps
If your pain IS in the normal range but you want to manage it better:
NSAIDs (ibuprofen, naproxen): Most effective when taken BEFORE pain peaks — start at the first sign of your period or even the day before if your cycle is predictable. They work by blocking prostaglandin production.
Heat: A heating pad on the lower abdomen is as effective as ibuprofen in some studies. Not a myth — actual measured pain relief.
Exercise: Counter-intuitive but effective. Physical activity increases blood flow and releases endorphins. Even a 20-minute walk helps.
Magnesium: Some evidence that magnesium supplements reduce cramp severity. Not dramatic but measurable.
Hormonal birth control: Reduces or eliminates period pain by suppressing ovulation and thinning the uterine lining. Very effective but comes with its own considerations.
What doesn’t work: “Just dealing with it” when simple treatments exist. Suffering unnecessarily isn’t a virtue.
Key Takeaways
- Some period pain is normal — mild to moderate cramping in the first 1–2 days that responds to ibuprofen.
- Pain that prevents normal functioning, gets worse over time, or has unusual features is NOT normal — it’s a signal.
- Endometriosis affects 10% of women and takes an average of 7–10 years to diagnose. It’s massively under-recognized.
- If your doctor dismisses severe pain as “just cramps” — push back. Request imaging, request a specialist referral.
- NSAIDs work best when taken early — before pain peaks, not after.
- Heat is genuinely effective — not just comforting, but measurably pain-reducing.
- Progressive pain (getting worse each cycle) is always worth investigating.
Sources
- Zondervan KT, et al. “Endometriosis.” New England Journal of Medicine, 2020.
- Armour M, et al. “The prevalence and academic impact of dysmenorrhea.” Journal of Women’s Health, 2019.
- Marjoribanks J, et al. “Nonsteroidal anti-inflammatory drugs for dysmenorrhea.” Cochrane Database of Systematic Reviews, 2015.
- Afshar Y, et al. “Adenomyosis.” Obstetrics and Gynecology Clinics of North America, 2017.
- Stewart EA. “Uterine Fibroids.” New England Journal of Medicine, 2015.
- Ballard K, et al. “What’s the delay? A qualitative study of women’s experiences of reaching a diagnosis of endometriosis.” Fertility and Sterility, 2006.
This article is for educational purposes only and does not constitute medical advice. If you have concerns about your health, please consult a qualified medical professional.
Don't leave it to the algorithm.
One article, straight to your inbox, whenever we publish. Written for humans, backed by research, free of clickbait.
Zero spam. One click to leave. Your inbox, your rules.