You’ve probably heard the name PCOS thrown around. Maybe a doctor mentioned it. Maybe you Googled your symptoms — irregular periods, acne that won’t quit, hair where you don’t want it — and it came up. Maybe someone told you it means you can’t have children.
Most of what gets shared about PCOS online is either oversimplified or outright wrong. So let’s start from scratch and build a real understanding — in plain language, with actual science, no medical jargon wall.
What PCOS Actually Is
PCOS stands for Polycystic Ovary Syndrome. The name is misleading in two ways:
-
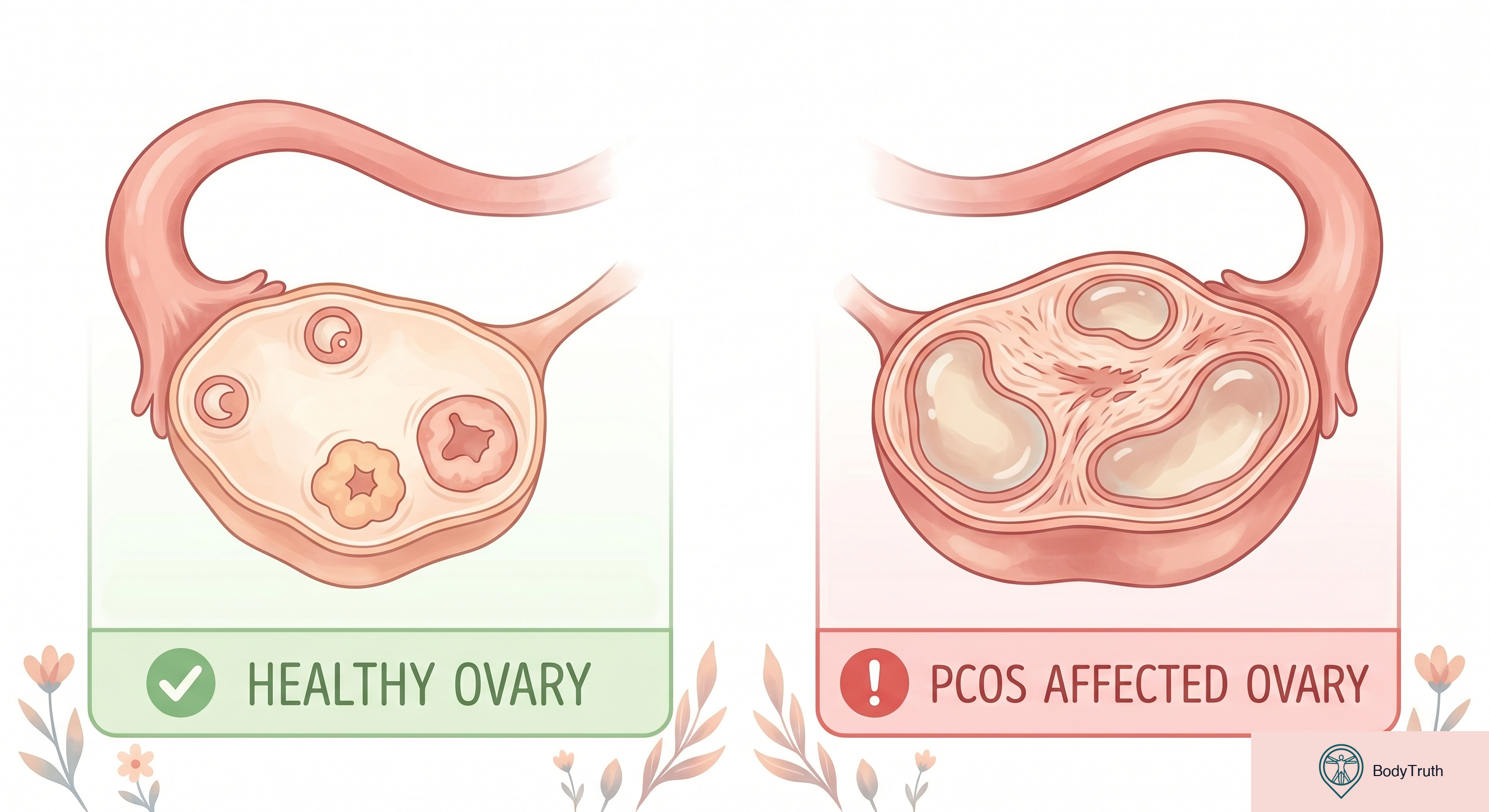
“Polycystic” suggests your ovaries are full of cysts. They’re not. What you have are follicles — tiny fluid-filled sacs that are a normal part of ovulation. In PCOS, more of these follicles develop than usual, but they often don’t mature enough to release an egg. They’re not cysts in the dangerous sense.
-
“Syndrome” means it’s a collection of symptoms, not a single disease. Not everyone with PCOS has the same symptoms, and there’s no single test that confirms it.
What’s actually happening: Your body produces more androgens (male hormones like testosterone) than typical for a female body. This hormonal imbalance disrupts the normal ovulation cycle and causes the symptoms you’re experiencing.
It affects roughly 1 in 10 women of reproductive age. It’s one of the most common hormonal conditions in women — and one of the most under-diagnosed.
The Symptoms (Not All Women Get All of Them)
PCOS shows up differently in different people. Here’s the full list — you might have two of these or six:
Menstrual:
- Irregular periods (longer than 35 days between cycles)
- Very heavy periods
- No period at all for months
- Unpredictable timing
Hormonal (androgen-related):
- Acne, especially along the jawline and chin
- Excess hair growth on face, chest, or abdomen (hirsutism)
- Thinning hair on the scalp (androgenic alopecia)
- Oily skin
Metabolic:
- Weight gain, especially around the abdomen
- Difficulty losing weight
- Insulin resistance (your body doesn’t use insulin efficiently)
- Darkened skin patches (acanthosis nigricans) — usually neck, armpits, groin
Reproductive:
- Difficulty getting pregnant (but NOT infertility — more on this below)
- Multiple small follicles visible on ultrasound
How It’s Diagnosed
Doctors typically use the Rotterdam Criteria — you need at least 2 of these 3:
- Irregular or absent ovulation (shown by irregular periods)
- High androgen levels (blood test or visible signs like excess hair/acne)
- Polycystic-appearing ovaries on ultrasound
There’s no single blood test for PCOS. The diagnosis is based on a pattern of symptoms after ruling out other conditions (thyroid disorders, adrenal conditions, etc.).
Important: Many doctors are still under-educated on PCOS. If you have these symptoms and your doctor dismisses them — get a second opinion, ideally from an endocrinologist or gynecologist who specializes in hormonal conditions.
What Causes It?
Honestly? We don’t fully know. The current understanding:
Genetics — it runs in families strongly. If your mother or sister has it, your risk is much higher.
Insulin resistance — about 70% of women with PCOS have some degree of insulin resistance. Excess insulin tells the ovaries to produce more testosterone. This is why PCOS and weight gain are connected — but it’s NOT caused by being overweight. Thin women get PCOS too.
Inflammation — women with PCOS often have elevated inflammatory markers, which may stimulate androgen production.
It’s not your fault. It’s not caused by anything you did or didn’t do. It’s a hormonal condition with strong genetic components.
The Fertility Myth
Let’s address this directly because it causes enormous anxiety: PCOS does not mean you can’t have children.
PCOS is the most common cause of ovulatory infertility — meaning it can make getting pregnant harder because you ovulate less regularly. But “harder” is not “impossible.”
The reality:
- Many women with PCOS conceive naturally — it just might take longer
- Ovulation can be induced with medication (letrozole or clomiphene) with high success rates
- Lifestyle modifications (especially reducing insulin resistance) can restore ovulation in many cases
- IVF success rates for women with PCOS are generally good
If you’ve been told “you’ll never have children” because of a PCOS diagnosis — that doctor was wrong. Get better medical advice.
What Actually Helps (Evidence-Based)
1. Lifestyle changes (first-line treatment for most women)
Exercise: 150 minutes per week of moderate activity. This directly improves insulin sensitivity, which reduces androgen levels, which improves ovulation. It doesn’t need to be intense — walking counts.
Nutrition: Focus on reducing insulin spikes rather than just “eating less.” This means:
- More protein and fiber with each meal
- Fewer refined carbs and sugars
- Eating regularly (skipping meals worsens insulin resistance)
- No specific “PCOS diet” is proven superior — the key is blood sugar stability
Weight management: Losing even 5–10% of body weight (if overweight) can significantly improve symptoms. But this is NOT about being thin — it’s about reducing insulin resistance. Thin women with PCOS need different approaches.
2. Medications
Metformin — originally a diabetes drug, it improves insulin sensitivity. Often prescribed for PCOS with insulin resistance. Can help restore regular periods and reduce androgen levels.
Birth control pills — regulate periods, reduce androgens, improve acne and hirsutism. Don’t treat the underlying cause but manage symptoms effectively.
Spironolactone — blocks androgen effects. Used for acne and excess hair growth.
Letrozole/Clomiphene — ovulation induction for women trying to conceive.
3. What doesn’t work
- Detox teas (do nothing)
- Supplements without evidence (most “PCOS supplements” are marketing)
- Extreme dieting (worsens hormonal balance)
- Ignoring it and hoping it goes away (it doesn’t — but it is manageable)
One supplement with actual evidence: Inositol (specifically myo-inositol and D-chiro-inositol). Multiple studies show improvement in insulin sensitivity and ovulation. It’s not a cure, but it’s one of the few supplements with real research behind it for PCOS.
The Weight Conversation
This needs its own section because it’s where most women with PCOS feel the most shame.
PCOS makes it physiologically harder to lose weight. Insulin resistance means your body is more efficient at storing fat and less efficient at burning it. This is not a willpower issue. It’s metabolic.
If you have PCOS and you’ve been told to “just eat less and exercise more” by a doctor who doesn’t understand the condition — that advice is incomplete. You likely need to address insulin resistance specifically (through the strategies above) before standard weight loss approaches will work normally.
And here’s the other side: not all women with PCOS are overweight. Lean PCOS exists and is often under-diagnosed because doctors associate the condition with excess weight. If you’re thin but have irregular periods, acne, and excess hair growth — PCOS is still worth investigating.
Long-Term Considerations
PCOS isn’t just about periods and fertility. Left unmanaged, it’s associated with increased risk of:
- Type 2 diabetes (due to insulin resistance)
- Cardiovascular disease
- Endometrial cancer (due to infrequent periods — the uterine lining builds up without shedding)
- Sleep apnea
- Depression and anxiety
This isn’t meant to scare you. It’s meant to emphasize that PCOS is worth managing actively — not just when you’re trying to get pregnant, but as an ongoing health priority throughout your life.
Key Takeaways
- PCOS is a hormonal condition affecting 1 in 10 women. The name is misleading — you don’t necessarily have “cysts.”
- Symptoms vary widely — irregular periods, acne, excess hair, weight gain, and difficulty conceiving are all possible.
- It does NOT mean infertility. Most women with PCOS can conceive with appropriate support.
- Insulin resistance is central to most cases. Addressing it improves almost all symptoms.
- Exercise + blood sugar management is the most effective first-line approach.
- It’s not your fault and it’s not a weight issue alone — thin women get it too.
- It requires long-term management — not just when you want to get pregnant.
Sources
- Teede HJ, et al. “Recommendations from the international evidence-based guideline for the assessment and management of PCOS.” Human Reproduction, 2018.
- Legro RS, et al. “Diagnosis and treatment of PCOS: An Endocrine Society Clinical Practice Guideline.” Journal of Clinical Endocrinology & Metabolism, 2013.
- Moran LJ, et al. “Lifestyle changes in women with polycystic ovary syndrome.” Cochrane Database of Systematic Reviews, 2011.
- Unfer V, et al. “Effects of myo-inositol in women with PCOS.” Gynecological Endocrinology, 2012.
- WHO. “Polycystic ovary syndrome.” Fact sheet, 2023.
This article is for educational purposes only and does not constitute medical advice. If you have concerns about your health, please consult a qualified medical professional.
Don't leave it to the algorithm.
One article, straight to your inbox, whenever we publish. Written for humans, backed by research, free of clickbait.
Zero spam. One click to leave. Your inbox, your rules.